By Martin Kulldorff, Biostatistician, Epidemiologist, Professor of Medicine, Harvard Medical School, Boston
Among COVID-19 exposed individuals, people in their 70s have roughly twice the mortality of those in their 60s, 10 times the mortality of those in their 50s, 40 times that of those in their 40s, 100 times that of those in their 30s, 300 times that of those in their 20s, and a mortality that is more than 3000 times higher than for children. Since COVID-19 operates in a highly age specific manner, mandated counter measures must also be age specific. If not, lives will be unnecessarily lost.
To determine effective public health counter measures against COVID-19, it is important to know the population characteristics of the epidemic [1]. It has been widely reported that mortality rates among those diagnosed and hospitalized are higher in older age groups [2, 3], but to determine public health action, it is the mortality among those exposed or infected that is of primary importance. Absolute risk estimates are uncertain at this stage of the epidemic, due to asymptomatic infected individuals [4] and limited population based testing [1], but with reasonable assumptions about exposure, it is possible to obtain rough estimates of the relative risks in different age groups, as well as upper bounds for the absolute risks.
We consider two alternative exposure scenarios at the early stages of the outbreak in Wuhan, before any social distancing was in place. In Scenario A, the likelihood of being exposed was equal in all age groups. In Scenario B, those <70 had twice the exposure compared to ages 70-79, who in turn had twice the exposure of those 80 and older. The truth probably lies somewhere in between these two scenarios.
Using Wuhan data for the relative risk of a COVID-19 diagnosis after exposure (RRC|E) and national Chinese data for the relative risk of death after a diagnosis (RRD|C) [2], the estimated relative risk of death among those exposed is RR = RRC|E x RRD|C. The Wuhan data better reflect the pre-social distancing phase of the epidemic while the Chinese mortality data increase the sample size of diagnosed individuals, generating more reliable estimates.
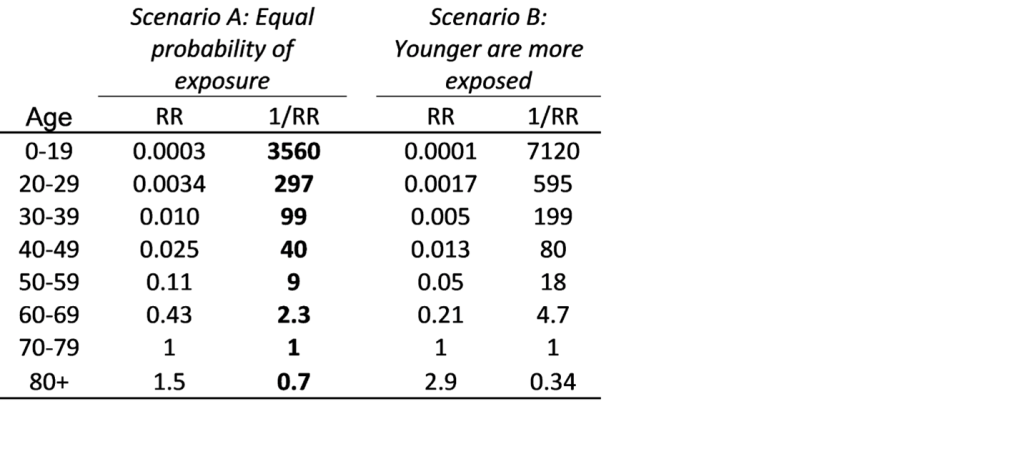
With age 70-79 as baseline, relative mortality risks are shown in Table 1. For COVID-19 exposed individuals, people in their 70s have roughly twice the mortality of those in their 60s, 10 times the mortality of those in their 50s, 40 times that of those in their 40s, 100 times that of those in their 30s, 300 times that of those in their 20s, and a mortality that is more than 3000 times higher than for children. Under Scenario B, with higher exposure among the young, the age differences are even larger.
In the United States, social distancing was in place early on, and since it is easier for retired people to stay home, it is likely that there was much less exposure among older people. Despite this, there is a higher proportion of diagnosed cases among the older population [5]. This means that the U.S. numbers are consistent with those from China.
Table 1: Relative risks (RR) for COVID-19 mortality by age group. In scenario A, pre-social distancing probability of exposure is assumed to be equal across all ages. In scenario B, it is assumed to be twice as high for those <70 and half as much for those >80, compared to age 70-79.
Since 1/RR is approximately 100 for age 30-39, exposure of only 1,000 people in their 70s would lead to the same number of deaths as the exposure of 100,000 persons in their 30s. In other words, in order to avoid the same fixed number of deaths, one must prevent COVID-19 exposure to 1,000 people in their 70s, or 10,000 people in their 50s, or 40,000 in their 40s, or 100,000 in their 30s, or 300,000 in their 20s, or 3.5 million children. Preventing exposure of 3.5 million children or 100,000 people in their 30s is practically, logistically, and financially more challenging than preventing exposure of 1,000 people aged 70-79.
Government officials would be wise to take advantage of these widely different mortality rates by age in devising their COVID-19 counter measures, while still maintaining essential societal services. Whether mandated counter measures are intensified, recalibrated, or gradually relaxed sometime in the future, age specific measures should be part of the strategy. If not, there will be unnecessary mortality, burden on hospitals and economic disruption. Counter measures directed specifically at older people will not only protect them, it will also free up health care resources for those younger people that do need hospital care.
To date, most government mandated mitigation measures have either been age neutral, such as restaurant closures, or targeted at young and middle-aged people, such as school and office closures. A more appropriate age targeted approach is needed. Just as some pubs ban customers under the age of 21, government officials could set temporary upper age limits of say 50, 60, or 65 for visiting or working at restaurants, stores, offices, airports, and other public places. So, for example, while all 60-plus-year-old supermarket cashiers, gas station attendants, police officers, postal workers, garbage collectors and bus drivers should stay home, their younger colleagues should keep working, taking extra shifts as needed.
Counter measures must consider not only relative risks but also absolute risks. Among diagnosed cases age 70-79, the mortality rate in China was 1 in 25. [2] Their absolute mortality risk when simply exposed is then less than that, although we do not know how much less. Transformed to other age groups, using the data from Table 1, the absolute risk-of-death point estimates among those exposed is less than 1 in 25×3560=89,000 for children, less than 1 in 7,500 for age 20-29, less than 1 in 2,500 for age 30-39, less than 1 in 1,000 for age 40-49, less than 1 in 230 for age 50-59, less than 1 in 58 for age 60-69, less than 1 in 25 for age 70-79 and less than 1 in 17 for those in the 80+ age group. These numbers for exposed individuals are more favorable but similar to recent mortality estimates for infected individuals [3]. To put these upper bounds in context, the upper bounds for children and young adults are lower than the U.S. infant mortality rate of 1 in 170 or the annual child mortality rate of around 1 in 6,000 [6]. For the older age groups, on the other hand, the upper bounds on the mortality rates are staggeringly high.
Infectious disease outbreaks have occurred throughout history and will continue to do so, aided by urbanization and long-distance travel. COVID-19’s ability to kill and its rapid spread make it a formidable enemy that is impossible to stop until herd immunity is reached. Just as in war, we must exploit the characteristics of the enemy in order to defeat it with the minimum number of casualties. Since COVID-19 operates in a highly age specific manner, mandated counter measures must also be age specific. If not, lives will be unnecessarily lost.
Martin Kulldorff, Biostatistician, Professor of Medicine, Harvard Medical School, Boston
References
[1] M. Lipsitch, D. L. Swerdlow och L. Finelli, ”Defining the Epidemiology of Covid-19 — Studies Needed,” New England Journal of Medicine, vol. 382, pp. 1194-1196, 2020.
[2] J. T. Wu, K. Leung, M. Bushman, N. Kishore, R. Niehus, P. M. d. Salazar, B. J. Cowling, M. Lipsitch och G. M. Leung, ”Estimating clinical severity of COVID-19 from the transmission dynamics in Wuhan, China,” Nature Medicine, pp. 1-5, 2020.
[3] R. Verity, L. C. Okell, I. Dorigatti, P. Winskill, C. Whittaker, N. Imai, G. Cuomo-Dannenburg och etal, ”Estimates of the severity of coronavirus disease 2019: a model-based analysis,” The Lancet Infectious Diseases, 2020.
[4] R. Li, S. Pei, B. Chen, Y. Song, T. Zhang, W. Yang och J. Shaman, ”Substantial undocumented infection facilitates the rapid dissemination of novel coronavirus (SARS-CoV2),” Science, nr March 16, 2020.
[5] CDC COVID-19 Response Team, ”Severe Outcomes Among Patients with Coronavirus Disease 2019 (COVID-19) — United States, February 12–March 16, 2020,” Morbidity and Mortality Weekly Report, vol. 69, nr 12, pp. 343-346, 2020.
[6] S. L. Murphy, J. Xu, K. D. Kochanek och E. Arias, ”Mortality in the United States, 2017,” National Center for Health Statistics, Hyattsville, MD, USA., 2018.
If we take human-caused global warming (AGW) as analogy, most of the world is already awakened to the fact that AGW is a fraud. For example, AGW is at the bottom of the list of concerns in surveys by the WHO. But WHO/UN management has AGW as a top priority as do over 100 governments.
AGW and pandemic fear mongering will stay as top priority for governments so long as voters continue electing politicians whose campaigns are funded by these special interests. AGW has been a political issue for over 30 years now, even though tens of thousands of scientists and thousands of peer review publications refute the AGW fraud.
Similarly, this virus “pandemic” is not about the science or disease, just as AGW is not about the science or the environment. Both are about politicians and government taking more control over people and resources; these are regressive political strategies, though supported by so-called “progressives,” promoted by revolutionaries and the communist/collectivist ideology to empower government control of everything. It will continue until voters throw them out of office.
Dr. Ryan Cole, pathologist, in the video at the link above essentially confirms the results of autopsies by pathologist Dr. Peter Schirmacher in Germany.
Dr. Peter Schirmacher, German pathologist, performed autopsies on 40 people who had died within two weeks of receiving a covid jab. Of those he autopsied, 30%-40% could be directly attributed to the “vaccines.” ‘In his opinion, the frequency of fatal consequences of vaccinations is underestimated…’ Dr. Schirmacher is world-renowned in his field, honored by The Pathologist as one of the 100 most influential in the world. He is the acting chairman of the German Society of Pathology, director of the Institute of Pathology at Heidelberg University Hospital, and president of the German Association for the Study of the Liver.
by Professor Hermann Harde, Experimental Physics and Materials Science, Helmut-Schmidt-University, Hamburg, Germany
Abstract: (link to full paper below. Published June 12, 2019)
The Intergovernmental Panel on Climate Change assumes that the inclining atmospheric CO2 concentration over recent years was almost exclusively determined by anthropogenic emissions, and this increase is made responsible for the rising temperature over the Industrial Era. Due to the far reaching consequences of this assertion, in this contribution we critically scrutinize different carbon cycle models and compare them with observations. We further contrast them with an alternative concept, which also includes temperature dependent natural emission and absorption with an uptake rate scaling proportional with the CO2 concentration. We show that this approach is in agreement with all observations, and under this premise not really human activities are responsible for the observed CO2 increase and the expected temperature rise in the atmosphere, but just opposite the temperature itself dominantly controls the CO2 increase. Therefore, not CO2 but primarily native impacts are responsible for any observed climate changes.
Hermann Harde, What Humans Contribute to Atmospheric CO2: Comparison of Carbon Cycle Models with Observations, Earth Sciences. Vol. 8, No. 3, 2019, pp. 139-159. doi: 10.11648/j.earth.20190803.13
I will also post here links to all of the materials he mentions on the thumb drive.
This is about 5 minutes and fast paced. His presentation was 7 August 2021. Entire board meeting (1 hour) is also recorded. In case you want this context, please let me know.
I think you will find this case interesting and informative, especially this ‘friends of the court statement” which is Attachment A on the court docket. This is a current case which will probably go to the U.S. Supreme Court. This and extensive references and many more important points are found at the link below.
Dr. Jay Bhattacharya is a Professor of Medicine at Stanford University and a research associate at the National Bureau of Economic Research. He is also Director of Stanford’s Center for Demography and Economics of Health and Aging. He holds an M.D. and Ph.D. from Stanford University. He has published 152 scholarly articles in peer-reviewed journals in the fields of medicine, economics, health policy, epidemiology, statistics, law, and public health, among others. His research has been cited in the peer-reviewed scientific literature more than 11,000 times.
Dr. Martin Kulldorff is a Professor of Medicine at Harvard Medical School, and he is a biostatistician and epidemiologist at Brigham and Women’s Hospital. He holds a Ph.D. from Cornell University. He is the author of 237 published articles in leading medical, epidemiological, statistics, and science journals, cited over 25,000 times in peer-reviewed scientific journals. Dr. Kulldorff is recognized internationally for his foundational research on the monitoring of vaccines and other medical health and safety issues. His methods are routinely used by the Centers for Disease Control and Prevention (“CDC”) and other public health agencies around the world.
Below is a teaser to attract your interest, but there is much more in this Attachment A and the other exhibits and the case itself. We live in interesting times.
“Multiple extensive, peer-reviewed studies comparing natural and vaccine immunity have now been published. These studies overwhelmingly conclude that natural immunity provides equivalent or greater protection against severe infection than immunity generated by mRNA vaccines (Pfizer and Moderna).” (Page 7 Attachment A.)
Abstract: …”Here we show that vaccines designed to reduce pathogen growth rate and/or toxicity diminish selection against virulent pathogens. The subsequent evolution leads to higher levels of intrinsic virulence and hence to more severe disease in unvaccinated individuals. This evolution can erode any population-wide benefits such that overall mortality rates are unaffected, or even increase, with the level of vaccination coverage. These findings have policy implications for the development and use of vaccines that are not expected to provide full immunity, such as candidate vaccines for malaria.”
~S Gandon 1 , M J Mackinnon, S Nee, A F Read, Institute of Cell, Animal and Population Biology, The University of Edinburgh, Edinburgh EH9 3JT, UK.
Nature.2001 Dec 13;414(6865):751-6. doi: 10.1038/414751a.
In other words, the medical and scientific community and the world have known for 20 years that vaccines which only treat symptoms without terminating the virus result in more infectious and dangerous disease and higher overall deaths. This is the Antibody-Dependent Enhancement (ADE) and immune escape described by brave doctors and scientists who are being blocked by social and mainstream media and ignored by governments and others with sworn duty to protect public health.



You must be logged in to post a comment.